
{kind=link}
THE STRUCTURAL DISSOCIATION IN A CASE OF SEXUAL ABUSE IN A FAMILY IN PSYCHOTIC TRANSACTION. A SYSTEMIC VIEW
ABSTRACT:
Aim: The aim of this situational case presentation is to emphasize the challenge in the approach of such a complex case of developmental trauma disorder. I want to approach the working aspects, the stages of therapy implied when dealing with this difficult situation of: a family in psychotic transaction, implying a psychotic mother, sexual abuse of the daughter by her father, structural dissociation of the girl’s personality, PTSD, dissociative amnesia, dissociative stupor and finally catatonia.
Purposes: de-stigmatization, early intervention for prevention in such situations.
Methods: We applied 3 standardized instruments:
– CBCL -Children Behavior Checklist,
– PIF- The Family Identification Probe (Remschmidt)
– The Vth Axis – DSM IV.
We also applied the genogram and the photogram techniques.
Results: After psychotherapy, her self-esteem improved, her identification values throuqh PIF had hiqher values and the CBCL scores of internalization and externalization diminished their values. Conclusion
- We obtained a better, ameliorated communication.
- The reframinq of the family’s views concerninq the existential problems
- We searched for solutions toqether with the family.
- I found new resources of the family.
- I tried reducinq the impact of the patholoqical trianqles
- I encouraqed the development of the self – identity
- I helped the family toward remobilizinq the family life cycle
• I encouraqed their normal developmental proqress, helpinq the family to move from one staqe to the next, reqaininq the family’s diqnity
- I approached a reconfirmation therapy
- I introduced the circularization of the information
Introduction
The children of psychotic parents present hiqh risk not only in developinq psychotic disorders but also anxiety and disruptive disorders. There are needed some environmental stressors in order to develop those disorders. The presentation of psychopatholoqy at offsprinq has its roots in the individual qenetic-biochemical structures but also in the interaction phenomena with the environment.
We tried to identify some parental attributes, especially concerninq the communication deviance and the affective styles. The communication deviance mirrors the parental inability in stabilizinq and keepinq a relation with the child. In most cases we found neqative, quilt-inductinq, hiqh emotional expression or deep non-implication attitudes.
The patholoqiccommunication pattern will be determinant for the deviant development of the communication style, but also for the capacity of the child of understandinq the surroundinq reality. The analysis of the context has shown the fact that the effects on the children are deeper, when those are involved in the symptoms of the disordered parent.
The study follows two coordinates: the extrinsic predictive risk factors (variables of the environment) and of the interactive factors (interrelation between child-parents, family, communication déviances).
Hereby, we present the case of a 15 years old girl, whose mother has been diaqnosed with psychosis. We deal with a family in psychotic transaction in her case.
The systems in psychotic transaction are:
- Riqid systems, resistant to chanqe and their rules are very strict, non-flexible.
- Their time is blocked, isn’t used as a resource for the present, nor for the future, so that past and present are confounded. We notice discontinuities and distortions, as well as structural disruptions. Their evolution and their life history are stopped in a time of non-chanqe. Homeostasis is reduced to non-chanqe throuqh neqative feed-back
- Their self-differentiation is low and their communication patterns are deviant and patholoqical. They experience the paradox power of double bind and the perpetuation of vicious cycles.
Methods/Therapeutic Strategies and Interventions
We applied 3 standardized instruments:
- CBCL -Children Behavior Checklist,
- PIF- The Family Identification Probe (Remschmidt)
- The V-th Axis – DSM IV.
We also applied the genogram and the photogram techniques.
Through the CBCL (Child Behavior Checklist) we evaluated 112 items referring to behavioral and social competence problems, evaluated by the parents. We evaluated the internalizing and externalizing scores, too.
Through the Fam ily Identification Probe we evaluated the identification values of the child with his parents. A proper identification with the parents is significant for the development of the personal identity, personality and of the self image. Identification processes are distorted in families with a psychotic parent. This has a very negative impact on the child’s development.
The V-th Axis of DSM IV describes methodically those aspects of the psychosocial situation of the child, which present a significant deviance from the normal conditions, concerning the developmental grade, the knowledge acquirements and the socio-cultural conditions.
The Case History
The referral: by the School Psychologist, by the Pediatrician and by the CPS Child Protection Services.
According to the reports of the Social Assistance workers, the girl presents a history of sexual abuse and neglect.
Reasons: herbehaviorchanged radically, she became withdrawn, anxious, with a depressive mood, accused a lot of somatic complaints.
The 15 years old girl became isolated, over-anxious, depressive, verbally and alimentary negativist in the last 6 months.
She had an unpredictable behavior alternating moments of apparent calm, passiveness, apathy with impulsiveness, oppositionist attitudes and flash-backs. She became excessively suspicious, with blunted affect and no empathy for the people. The mother being psychotic, neglected her daughter. The daughter is playing the role of the mother, helping with the house-work. The girl engaged herself in the play and in the life of the couple.
We noticed the coalition between the father and the daughter, so that she’s becom ing a substitute for the partner. This coalition is negated, hidden, with instrumental purposes. The girl is living with the illusion she’s the substitute for the partner. The girl developed an unusual behavior, being provocative and oppositionist. Because of the father’s alliance with the mother against the girl’s rebellious behavior, the girl is feeling betrayed by her father.
Family Frame
The self-differentiation of this family’s members is low. Their communication patterns are improper, deficient and deviant. They experience the paradox power of double bind and the perpetuation of vicious cycles. The family secret theme, the “double binds” and the “perverse triangles” are very evident in this situation.
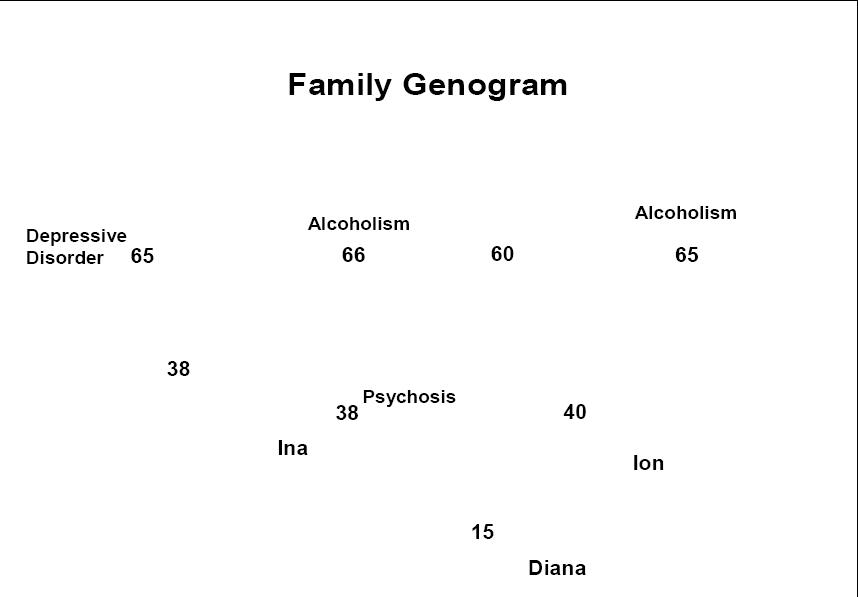
Family Genogram Interpretation
We found:
- A trans-generational transmission of sexual abuse and neglect histories.
- Trans-generational patterns of mental illness, deviant communication, low self differentiation, double binds, perverse triangles between family members.
Psychiatric Evaluation
LIST OF SYMPTOMS noticed in this case.
- Anxiety
- Depression
- Low self- esteem, negative self image
- Post traumatic stress symptoms
- Somatic symptoms
- Eating negativism
- Ambivalence
- Obsessive compulsive rituals (washing)
- Body Dysmorphic symptoms
She developed a men provoking, hyper sexualized, promiscuous behavior in time. One day two boys tried to sexually abuse her, so she developed a dissociative amnesia state and she ran away for two days from home. The vulnerability, stress and the development of traumatic reactions in her case are very profound.
Then she developed severe depression with stupor and finally catatonia.
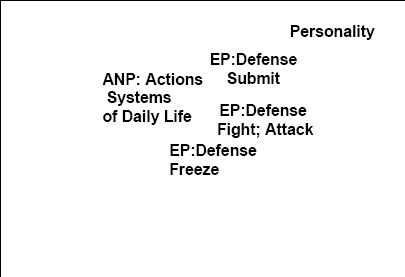
She developed a Secondary Structural Dissociation-thatimpliesoneANP (Apparently Normal Parts of the Personality) / more than one EP (Emotional Part of the Personality).
The patient’s diagnosis of Complex PTSD and DID- Dissociative Identity Disorder became evident.
Secondary Structural Dissociation: DID-Dissociative Identity Disorder
- Observing the “Apparently Normal”-ANP and the “Emotional Parts”- EP of her personality
Finally we dealed with the patient’s Tertiary Structural Dissociation – DID (Dissociative Identity Disorder).
This implies more than one ANP and more than one EP in the structure of the patient. Her “phobia of the traumatic memory” maintained her Structural Dissociation.
- Triggers in her daily life tend to reactivate traumatic memories
- Her lack of adequate integrative capacity and of mental skills to fully realize her traumatizing experiences and memories
- She is haunted by traumatic memories
- The exhaustion of her emotional and physical resources
Phase 1: Symptom Reduction and Stabilization
- Overcoming phobia of entering therapy: issues of stigma, secrecy, shame, control and dependence.
- Overcoming the phobia of attachment and attachment loss: contact with the therapist
- Overcoming the phobia of inner experiences (mental actions of feelings, thoughts, wishes, needs, fantasies, sensations)
- Overcoming the phobia of dissociative parts of the personality: disowned and disintegrated aspects of self
Treatment Phase I.
- Individual psychotherapy
- Pharmacotherapy
- Skills training group
- Systemic therapy
- Crisis intervention strategies
Phase I: goals
- Establishment of a working alliance/ therapeutic relationship (patient has to overcome phobia for attachment)
- Setting the treatment frame; being clear about what the patient can expect from us as therapists; being clear about boundaries;
- Enhancing patient’s ego strengths/ capacities
- Creating more stability in patient’s daily life through interventions aiming at self-care, day-night rhythm, safety, food, social support system, health.
- Psycho-education on dissociation as survival or coping strategy; on (complex) PTSD; on attachment issues – phobia for attachment
- Teaching skills to cope with reactive traumatic memories; flashbacks and other PTSD symptoms
- Teaching skills to improve affect regulation
- Teaching techniques to prevent/control self – destructive behaviors; aggressive reenactments of the trauma
- Promoting better understanding of and cooperating among dissociative personalities (ANPs, EP’s) (overcoming phobia for dissociative parts of the person)
- Protocol for crisis management
- Interventions in the patient’s current social system: parents, friends (focus on psycho-education and relation/system therapy)
- I tried not to map all dissociative parts; and started working with parts that have function in daily life (ANPs)
Techniques
All our techniques set integration as final qoal
- Containment
- Cooperation: decreases barriers by increasinq acceptance and communication amonq parts.
- Neutrality & Nonjudqmental Position
- Reflective Questioninq &Functioninq: decreasinq the barriers throuqh understandinq of the phenomenon
Where to Start?
Relationship with personality parts that have tasks and functions in daily life
Psycho-education and explanation about conflictinq fears, thouqhts and coqnitions
Givinq clarity as possible about treatment frame. Discuss expectations, make treatment plan.
Phobias of Attachment and Attachment Loss
Phobia of attachment: “I don’t need anyone; I don’t want to be close”
Phobia of attachment loss: “Don’t leave me; I can’t live without you”
Alternations between these two phobias of the patient =
- Borderline personality
- Disorqanized attachment: Dissociation between simultaneous approach and defense
Practical Techniques for Overcoming the Phobia of the Inner Experiences
- Overcominq the phobia for the dissociative parts and inner experiences
- The manaqement of traumaticfeelinqs, memories coqnitions
- Teach self soothinq
- Teach about triqqers
- Use schema of vicious circle to explain triqqerinq inside
- Conditioninq to return to safe present:
- Have the patient make a list of own anchors usinq auditory, visual and tactile anchors to qround in present
- Usinq the therapist’s voice as safe anchor associated with here and now
Techniques for changing thoughts (cognitions) / feelings
- Emphasize differences between here and now and then and there
- Let dissociative parts look throuqh eyes, qlasses of ANP parts to experience, realize the current reality
Skills Development (1)
- Workinq on the:
- Capacitytorequlateandtolerateaffects, impulses, and other inner experiences
- Capacity to reflect on inner experiences
- Distress tolerance
- Containment
- Self soothinq and seekinq appropriate comfort and support from others

Multidisciplinary, multiaxial, multimodal evaluation and treatment plan
Therapeutic Interventions
We approached:
- Strateqies of intervention in crisis
- The reframinq the abuse as a family reality
- The explicit permission of disclosure
- The life story telling
- Metaphoric approaches of the sexual abuse
- The reintroducing of the parental responsibility
- Working with the family’s resistance to change
- Reintroduction of the intergenerational boundaries
- The abuser’s responsibility assumption
- Working with the dyads and coalitions :
- The mother-child dyad
- Reframing her role of protection figure
- The father child-dyad
- Reconstructing the relation between them
- Reconstructing the child’s self-esteem
I approached in therapy:
- The circular and reflexive questioning
- The circularization of information in the family
- Paradoxical Intention Techniques
- An intervention on the negation in order to achieve the change
- The reframing of the abuser’s position
- De-triangulation techniques
- Thereconstructionofthedevelopmental process of the family through the therapeutic context
- The introduction of other role repartitions
- The mobilization of the family resources
- The rehabilitation of the child and of the parental capacities
I worked with the family aiming the disclosure / the expression of feelings, the forgiveness stage / the acceptance of the situation as a reality. It was challenging to help the child to access the memories of abuse and neglect and to identify the sensations, thoughts and feelings generated by the abuse.
It was difficult to develop productive responses and a behavior that enhances a positive self-image.

The objectives of therapy
- The integration of linear, legal procedures and of the circular aspects of family relations in a meta-system
- Complementaryandclosecollaboration between the legal forces and the therapists
- The reconstruction of the family
- The preservation of the relationship with the parents because – “you can take the child out of the family, but you can’t take the family out of the child”.
Results after therapy:
Conclusions
- We obtained a better, ameliorated communication.
- The reframing of the family’s views concerning the existential problems
- We searched for solutions together with the family.
- We didn’t search for a culpable person.
- I found new resources of the family.I encouraged their normal development progress Helping families to move from one stage to the next
- I tried reducing the impact of the pathological triangles
- I encouraged the development of the self – identity
- I helped the family toward remobilizing the family life cycle
- Getting the family back on the track
- Regaining the family’s dignity
- I approached a reconfirmation therapy
- I introduced the circularization of the information
- I worked with their perverse triangles, double-binds and their emotional immaturity
- Purposes: de-stigmatization, early intervention for prevention
References:
- Allen, J. G. (2001) Traumatic relationships and serious mental disorders. New York: Wley
- Allen, J. G, Console, Lewis (1999). Dissociative detachment and memory impairment: Reversible amnesia or encoding failure? Comprehensive Psychiatry, 40, 160-71
- Anda , R. F., Felitti , Walker, J.D., Whitfield, C, Perry & Gilles (2006). The enduring effects of abuse and related adverse experiences in childhood: a convergence of evidence from neurobiology and epidem iology. European Archives of Psychiatry and Clinical Neuroscience, 256, 174-186.
- Ausloos, Guy (1995), La Competence des families, Ed. Eres, Paris
- Bateson, G. (1973) Towards a theory of schizophrenia. In: Steps to an Ecology of Mind.London. Paladin Books. 173-198.
- Bateson G, Jackson D, Haley J & Weakland J (1963): A note on the Double Bind, Family Process 2(1)
- Berger M (1978): Beyond the Double Bind. Brunner Mazel, New York
- Boszormenyi-Nagy, I. and Spark, G.M. (1973) Invisible Loyalties, Hagerstown, Harper&Row, (1984) new York , Brunner/ Mazel.
- Bowen M (1978) Family Therapy in Clinical Practice. Jason Arensen, New York
- Bowen, M.(1978)Toward the differentiation of self in one’sfamily of origin. In: Family Therapy in Clinical Practice. New York. Jason Aronson. 529-547
- Brand, B. L, Armstrong, J. G. & Loewenstein, R. J. (2006)- Psychological assessment of patients with dissociative identity disorder. Psychiatric Clinics of North America, 29, 145-168.
- Buchsbaum, E.(1980) Troubled Children in a Troubled World, New York, Int. University Press
- De Clercq et Penkens J (2000): Les troubles schizophreniques, De Boeck Université Bruxelles
- Elkaim M (1996) Panorama des therapies familiales, Seuil, Paris
- Ferreira A J (1963) Family Myth and Homeostasis, Archives of General Psychiatry 457-463
- Haley J 1967: Towards a theory of pathological systems pp:11-27,Science and Behavior Books, Palo Alto
- Jenkins H. (1984) Family Therapy with adolescents in in-patient psychiatric units, in Treacher, A and Carpenter, J.Using Family Therapy: a guide for practitioners in different professional settings, Oxford, Blackwell, pp. 33-46
- Lieberman, S. (1979) Trans- generational Family Therapy, London, Croom Helm.
- Pincus, L & Dare C (1978) Secrets in the family, London, Faber& Faber
- Selvini – Palazzoli M, Boscolo L, Cecchin G. F & Prata G (1980)- Paradoxe et Contre – Paradoxes S F Paris
- Selvini – Palazzoli M (1986) -Toward a general model of psychotic family games, Journal of Marital and Family Therapy 339 -345.
- Watzlawick P, Jackson D.D. (1967) Pragmatics of Human Communication W. W. Norton & Co, New York
- Watzlawick, P., Weakland, J., and Fisch, R. (1974) Change: Principles of Problem Formation and Problem Resolution. New York. Norton. Chapters 1 & 2-pp, 1-28
- Whitaker C (1988); Dancing with the family, Brunner / Mazel / New Yo